Introduction: Pediatric lower extremity burns pose a significant challenge due to their impact on physical function, aesthetics, and quality of life. This study aims to assess the incidence, severity, management approaches, and outcomes of lower limb burns in children within the context of Bangladesh. Methods: This prospective observational study was conducted in the Department of Burn and Plastic Surgery, Dhaka Medical College Hospital, Dhaka, Bangladesh, from January 2021 to October 2022. In this study, a total of 40 pediatric patients with lower extremity burns were analyzed. Result: The most affected age group was 5–8 years (35%), with a higher prevalence in females (62.5%). Scald burns were the most common cause (35%), followed by flame burns (30%). Superficial partial-thickness burns were the most frequent (37.5%). Surgical intervention was required in 47.5% of cases, predominantly for flame and ash burns. Common surgical procedures included wound excision, scar release, and skin grafting. Delayed hospital admission beyond five days occurred in nearly half of the cases. Functional outcomes varied, with full range of motion achieved in 50% of patients and full functionality restored in 25%. Surgical cases had a higher incidence of hypertrophic scarring and limited functionality. Conclusion: Pediatric lower extremity burns require a multifaceted approach, with early intervention crucial in reducing complications. Delayed admissions contribute to worse outcomes, highlighting the need for improved burn awareness and timely medical intervention.
| Published in | American Journal of Health Research (Volume 13, Issue 2) |
| DOI | 10.11648/j.ajhr.20251302.12 |
| Page(s) | 92-101 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Lower Extremity Burns, Children, Incidence, Bangladesh
Baseline Characteristics | Frequency (n) | Percentage (%) |
|---|---|---|
Age range | ||
6 month-2y | 11 | 4.4% |
2y-5y | 7 | 17.5% |
5y-8y | 14 | 35% |
8y-11y | 4 | 10% |
11y-14y | 4 | 10% |
Sex | ||
Male | 15 | 37.5% |
Female | 25 | 62.5% |
Causes of burn | ||
Scald | 14 | 35 |
Ash burn | 5 | 12.5 |
Flame burn | 12 | 30 |
Electrical burn | 3 | 7.5 |
Tar burn | 2 | 5 |
Chemical Burn | 2 | 5 |
Friction Burn | 2 | 5 |
Depth of burn | ||
Superficial partial thickness | 15 | 37.5 |
Deep partial thickness | 9 | 22.5 |
Deep | 7 | 17.5 |
Mixed | 9 | 22.5 |
Side affected | ||
Right | 16 | 40 |
Left | 13 | 32.5 |
Both | 11 | 27.5 |
Location of defect | ||
Flexor | 16 | 40 |
Extensor | 13 | 32.5 |
Both | 11 | 27.5 |
Dressing material | Frequency | Percentage (%) |
|---|---|---|
Silcream | 8 | 20 |
Hydrocolloid + gypsonet & povidone Iodine ointment | 7 | 17.5 |
Gypsonet & povidone Iodine ointment | 10 | 25 |
Silcream + Gypsonet & povidone Iodine ointment | 5 | 12.5 |
Hydrocolloid | 6 | 15 |
Hypochlorous acid solution(Mizouh) | 2 | 5 |
Alginate+ absorbent gel (Flaminol) | 2 | 5 |
Surgery | Frequency | Percentage (%) |
|---|---|---|
Needed | 19 | 47.5 |
Not needed | 21 | 52.5 |
Burns that needed surgery | ||
Ash burn | 5 | 12.5 |
Flame burn | 7 | 17.5 |
Tar burn | 2 | 5 |
Scald | 3 | 7.5 |
Friction burns | 2 | 5 |
Cause of burn | Wound excision | Scar release | Primary closure | Split-thickness skin graft | Full-thickness skin graft | Total procedure |
|---|---|---|---|---|---|---|
Ash burn | 5 | 3 | 1 | 5 | 2 | 16 |
Flame burn | 7 | 2 | 1 | 4 | 2 | 16 |
Tar burn | 2 | 1 | 1 | 2 | nil | 6 |
Scald | 3 | nil | nil | 3 | nil | 6 |
Friction burn | 2 | nil | nil | 2 | nil | 4 |
The gap in days between burn and hospital admission | Frequency | Percentage (%) |
|---|---|---|
Same day | 11 | 27.5 |
1 day | 7 | 17.5 |
2 days | 2 | 5 |
3 days | 3 | 7.5 |
5 days | 4 | 10 |
7 days | 3 | 7.5 |
8 days | 4 | 20 |
11 days | 1 | 2.5 |
14 days | 2 | 5 |
30 days | 3 | 7.5 |
Patient Outcomes | All | Surgical | Nonsurgical |
|---|---|---|---|
Total patients | 40 | 19 | 21 |
Scar contracture | |||
None | 15 | 4 | 11 |
Minimal | 14 | 10 | 4 |
Severe | 11 | 11 | Nil |
Scar quality | |||
Good | 14 | 2 | 12 |
Hypertrophic | 9 | 6 | 3 |
Hyperpigmented | 7 | 3 | 4 |
Immature | 11 | 4 | 7 |
ROM | |||
Full | 20 | 8 | 12 |
Limited | 10 | 5 | 5 |
Unknown | 10 | 5 | 5 |
Functionality | |||
Full | 10 | 4 | 6 |
Limited | 15 | 10 | 5 |
Unknown | 15 | 5 | 10 |
Type of burn | Total patients | Surgery needed | 2 weeks | 4 weeks | 6 weeks | Surgery not needed | 2 weeks | 4 weeks | 6 weeks |
|---|---|---|---|---|---|---|---|---|---|
Scald | 14 | 3 | 5 | 8 | 3 | 11 | 10 | 2 | nil |
Ash burn | 5 | 5 | 4 | 5 | 2 | ||||
Flame burn | 12 | 7 | 5 | 7 | 8 | 5 | 4 | 3 | 3 |
Electric burn | 3 | nil | nil | nil | 3 | 3 | 2 | nil | |
Tar burn | 2 | 2 | 1 | 2 | 1 | nil | |||
Chemical burn | 2 | nil | nil | nil | nil | 2 | 2 | 1 | 1 |
Friction burn | 2 | 2 | 2 | 1 |
Type of burn | Surgery needed | Surgery not needed | Parameter | Description | Points | Score in no. of surgical pts(3) | Score in nonsurgical pts(11) | Total points in surgical pts | Total points in nonsurgical pts |
|---|---|---|---|---|---|---|---|---|---|
Scald(14) | 3 | 11 | pigmentation | Normal | 0 | nil | 8 | 2 | 1 |
hypopigmented | 1 | nil | 3 | ||||||
hyperpigmented | 2 | 3 | nil | ||||||
vascularity | Normal | 0 | nil | 8 | 1 | 3 | |||
Pink | 1 | 1 | 2 | ||||||
Red | 2 | nil | 1 | ||||||
Purple | 3 | 2 | nil | ||||||
pliability | Normal | 0 | nil | 8 | 0 | 7 | |||
Supple | 1 | nil | nil | ||||||
Yielding | 2 | nil | nil | ||||||
Firm | 3 | 2 | nil | ||||||
Banding | 4 | 1 | nil | ||||||
Contracture | 5 | nil | nil | ||||||
Height | Normal(flat) | 0 | nil | 8 | 0 | 3 | |||
>0 and <2 mm | 1 | 2 | nil | ||||||
>2mm and<5mm | 2 | 1 | nil | ||||||
>5 mm | 3 | nil | nil |
DMCH | Dhaka Medical College and Hospital |
ROM | Range of Motion |
TBSA | Total Body Surface Area |
STSG | Split-Thickness Skin Graft |
FTSG | Full-Thickness Skin Graft |
| [1] | Heimbach D. Burn patients, then and now. Burns. 1999; 25(1): 1-2. |
| [2] | Peden M, McGee K, Sharma G. The injury chart book: a graphical overview of the global burden of injuries. Geneva: World Health Organization; 2002. |
| [3] | Krug E. Injury surveillance is key to preventing injuries. Lancet. 2004; 364(9445): 1563-6. |
| [4] | Rivara FP. Burns: the importance of prevention. Inj Prev. 2000; 6(4): 243-4. |
| [5] | Mercier C, Blond MH. Epidemiological survey of childhood burn injuries in France. Burns. 1996; 22(1): 29-34. |
| [6] | Cronin KJ, Butler PEM, McHugh M, Edwards G. A 1-year prospective study of burns in an Irish paediatric burns unit. Burns. 1996; 22(3): 221-4. |
| [7] | Bang RL, Ebrahim MK, Sharma PN. Scalds among children in Kuwait. Eur J Epidemiol. 1997; 13(1): 33-9. |
| [8] | Mashreky SR, Rahman A, Chowdhury SM, Giashuddin S, Svanström L, Linnan M, Shafinaz S, Uhaa IJ, Rahman F. Epidemiology of childhood burn: yield of largest community based injury survey in Bangladesh. Burns. 2008 Sep 1; 34(6): 856-62. |
| [9] | Menon S, Ward D, Harvey JG, et al. Friction burns in children: does laser Doppler imaging have a role? J Burn Care Res. 2012; 33(6): 736-40. |
| [10] | World Health Organization. Burns fact sheet 2018. Available from: |
| [11] | Barbour JR, Schweppe M, O S-J. Lower-Extremity Burn Reconstruction in the Child. J Craniofac Surg. 2008; 19(4): 976-88. |
| [12] | Schneider JC, Holavanahalli R, Helm P, et al. Contractures in burn injury: defining the problem. J Burn Care Res. 2006; 27(4): 508-14. |
| [13] | Macarthur C. Evaluation of Safe Kids Week 2001: prevention of scald and burn injuries in young children. Inj Prev. 2003; 9(2): 112-6. |
| [14] | Forjuoh SN. Burns in low- and middle-income countries: a review of available literature on descriptive epidemiology, risk factors, treatment, and prevention. Burns. 2006; 32(5): 529-37. |
| [15] | van Baar ME, Essink-Bot M, Oen L, Dokter IMMH, Boxma J, Beeck H, et al. Functional outcome after burns: a review. Burns. 2006; 32(1): 1-9. |
| [16] | Chang FC, Herzog B. Burn morbidity: a follow-up study of physical and psychological disability. Ann Surg. 1976; 183(1): 34-7. |
| [17] | Tedstone JE, Tarrier N. An investigation of the prevalence of psychological morbidity in burn-injured patients. Burns. 1997; 23(6): 550-4. |
| [18] | Bowden LP, Royer MC, Hallman JR, et al. Rapid onset of argyria induced by a silver-containing dietary supplement. J Cutan Pathol. 2011; 38(9): 832-5. |
| [19] | Forjuoh SN, Guyer B, Ireys HT. Burn-related physical impairments and disabilities in Ghanaian children: prevalence and risk factors. Am J Public Health. 1996; 86(1): 81-3. |
| [20] | Engrav LH, Covey MH, Dutcher KD, Heimbach DM, Walkinshaw MD, Marvin JA. Impairment, time out of school, and time off from work after burns. Plast Reconstr Surg. 1987; 79(6): 927-34. |
| [21] | Staley M, Anderson L, Greenhalgh D, Warden G. Return to school as an outcome measure after a burn injury. J Burn Care Rehabil. 1999; 20(1): 91-4. |
| [22] | Bowden ML, Thomson PD, Prasad JK. Factors influencing return to employment after a burn injury. Arch Phys Med Rehabil. 1989; 70(9): 772-4. |
| [23] | Iregbulem LM. Postburn volar digital contractures in Nigerians. Hand. 1980; 12(1): 54-61. |
| [24] | Sankale AA, Manyacka Ma Nyemb P, Coulibaly NF, Ndiaye A, Ndoye M. Les cicatrices retractiles post-brulures du membre inferieur chez L’Enfant. Ann Burns Fire Disasters. 2010; 23(2): 75-80. |
| [25] | Sankale AA, Ndiaye A, Ndoye A, Ndiaye L, Ndoye M. Les séquelles de brûlures cervicocéphaliques chez l’enfant. Ann Burns Fire Disasters. 2011; 24(1): 34-8. |
| [26] | Suliman MT. Experience with the seven flap-plasty for the release of burns contractures. Burns. 2004; 30(4): 374-9. |
| [27] | Chukwuanukwu TOG, Opara KO, Nnabuko REE. Paediatric post-burn contractures in Enugu, Nigeria. Niger J Plast Surg. 2007; 3(1): 1-4. |
| [28] | Sankale-Diouf AA, Wandaogo A, Tekou H, Fall I, Ndoye M. Les cicatrices rétractiles de la main brûlée chez l’enfant: une revue de 79 cas. Ann Chir La Main Du Memb Super. 1999; 18(1): 21-7. |
| [29] | Meng F, Zuo KJ, Amar-Zifkin A, Baird R, Cugno S, Poenaru D. Pediatric burn contractures in low-and lower middle-income countries: a systematic review of causes and factors affecting outcome. Burns. 2020; 46(5): 993-1004. |
| [30] | Gupta S, Wong EG, Mahmood U, Charles AG, Nwomeh BC, Kushner AL. Burn management capacity in low and middle-income countries: A systematic review of 458 hospitals across 14 countries. Int J Surg. 2014; 12(10): 1070-3. |
| [31] | Ramakrishnan KM, Sankar J, Venkatraman J. Profile of pediatric burns: Indian experience in a tertiary care burn unit. Burns. 2005; 31(3): 351-3. |
| [32] | Nath S, Erzingatsian K, Simonde S. Management of postburn contracture of the neck. Burns. 1994; 20(5): 438-41. |
| [33] | Peleg K, Goldman S, Sikron F. Burn prevention programs for children: do they reduce burn-related hospitalizations? Burns. 2005; 31(3): 347-50. |
| [34] | Duzgun AP, Senel E, Ozmen MM, Kulacoglu H, Isik Y, Coskun F. Evaluation of the patients admitted to a burn center in Turkey. Turk J Trauma Emerg Surg. 2003; 9(4): 250-6. |
| [35] | Rouzbahani R, Omranifard M, Rouzbahani A, Barkhordari M. An epidemiological study on burned patients admitted in the burn hospital in Isfahan Province, Iran in 2002. Rawal Med J. 2004; 29(1): 13-7. |
| [36] | Song C, Chua A. Epidemiology of burn injuries in Singapore from 1997 to 2003. Burns. 2005; 31(Suppl 1): S18-26. |
APA Style
Chowdhury, R., Amin, M. S., Haque, M. M., Ahmed, I. (2025). Paediatric Lower Extremity Burns in Bangladesh: Incidence and Outcome. American Journal of Health Research, 13(2), 92-101. https://doi.org/10.11648/j.ajhr.20251302.12
ACS Style
Chowdhury, R.; Amin, M. S.; Haque, M. M.; Ahmed, I. Paediatric Lower Extremity Burns in Bangladesh: Incidence and Outcome. Am. J. Health Res. 2025, 13(2), 92-101. doi: 10.11648/j.ajhr.20251302.12
@article{10.11648/j.ajhr.20251302.12,
author = {Riffat Chowdhury and Mohammad Sadiqul Amin and Mohammad Mazharul Haque and Iqbal Ahmed},
title = {Paediatric Lower Extremity Burns in Bangladesh: Incidence and Outcome
},
journal = {American Journal of Health Research},
volume = {13},
number = {2},
pages = {92-101},
doi = {10.11648/j.ajhr.20251302.12},
url = {https://doi.org/10.11648/j.ajhr.20251302.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajhr.20251302.12},
abstract = {Introduction: Pediatric lower extremity burns pose a significant challenge due to their impact on physical function, aesthetics, and quality of life. This study aims to assess the incidence, severity, management approaches, and outcomes of lower limb burns in children within the context of Bangladesh. Methods: This prospective observational study was conducted in the Department of Burn and Plastic Surgery, Dhaka Medical College Hospital, Dhaka, Bangladesh, from January 2021 to October 2022. In this study, a total of 40 pediatric patients with lower extremity burns were analyzed. Result: The most affected age group was 5–8 years (35%), with a higher prevalence in females (62.5%). Scald burns were the most common cause (35%), followed by flame burns (30%). Superficial partial-thickness burns were the most frequent (37.5%). Surgical intervention was required in 47.5% of cases, predominantly for flame and ash burns. Common surgical procedures included wound excision, scar release, and skin grafting. Delayed hospital admission beyond five days occurred in nearly half of the cases. Functional outcomes varied, with full range of motion achieved in 50% of patients and full functionality restored in 25%. Surgical cases had a higher incidence of hypertrophic scarring and limited functionality. Conclusion: Pediatric lower extremity burns require a multifaceted approach, with early intervention crucial in reducing complications. Delayed admissions contribute to worse outcomes, highlighting the need for improved burn awareness and timely medical intervention.
},
year = {2025}
}
TY - JOUR T1 - Paediatric Lower Extremity Burns in Bangladesh: Incidence and Outcome AU - Riffat Chowdhury AU - Mohammad Sadiqul Amin AU - Mohammad Mazharul Haque AU - Iqbal Ahmed Y1 - 2025/03/06 PY - 2025 N1 - https://doi.org/10.11648/j.ajhr.20251302.12 DO - 10.11648/j.ajhr.20251302.12 T2 - American Journal of Health Research JF - American Journal of Health Research JO - American Journal of Health Research SP - 92 EP - 101 PB - Science Publishing Group SN - 2330-8796 UR - https://doi.org/10.11648/j.ajhr.20251302.12 AB - Introduction: Pediatric lower extremity burns pose a significant challenge due to their impact on physical function, aesthetics, and quality of life. This study aims to assess the incidence, severity, management approaches, and outcomes of lower limb burns in children within the context of Bangladesh. Methods: This prospective observational study was conducted in the Department of Burn and Plastic Surgery, Dhaka Medical College Hospital, Dhaka, Bangladesh, from January 2021 to October 2022. In this study, a total of 40 pediatric patients with lower extremity burns were analyzed. Result: The most affected age group was 5–8 years (35%), with a higher prevalence in females (62.5%). Scald burns were the most common cause (35%), followed by flame burns (30%). Superficial partial-thickness burns were the most frequent (37.5%). Surgical intervention was required in 47.5% of cases, predominantly for flame and ash burns. Common surgical procedures included wound excision, scar release, and skin grafting. Delayed hospital admission beyond five days occurred in nearly half of the cases. Functional outcomes varied, with full range of motion achieved in 50% of patients and full functionality restored in 25%. Surgical cases had a higher incidence of hypertrophic scarring and limited functionality. Conclusion: Pediatric lower extremity burns require a multifaceted approach, with early intervention crucial in reducing complications. Delayed admissions contribute to worse outcomes, highlighting the need for improved burn awareness and timely medical intervention. VL - 13 IS - 2 ER -
Department of Plastic and Reconstructive Surgery, Dhaka Medical College and Hospital, Dhaka, Bangladesh
Department of Orthopaedic Surgery, Gopalganj Medical College, Gopalganj, Bangladesh
Department of Plastic and Reconstructive Surgery, Dhaka Medical College and Hospital, Dhaka, Bangladesh
Department of Plastic and Reconstructive Surgery, Dinajpur Medical College, Dinajpur, Bangladesh
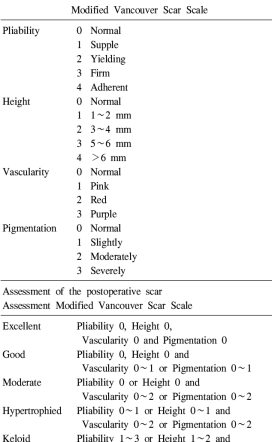
Figure 1. Modified Vancouver scar scale assessment.
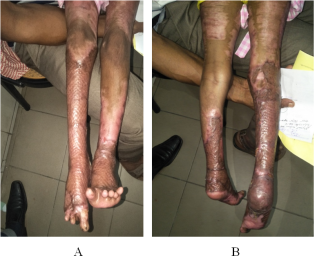
Figure 2. A): 20% ash burns both lower limbs, B) 6 months follow up picture (3 stages STSG done).

Figure 3. A): Flexion contracture of all toes released and FTSG done, B) 6 months follow-up picture (3 stages done).

Figure 4. (A &B): Chemical burn (immediate and 8th post-burn day).
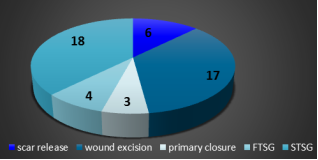
Figure 5. Distribution of pediatric patients by procedures.

